
Chest X-ray
📌 What is a Chest X-Ray?
A chest X-ray is a fast, non invasive imaging test used to visualise the lungs, heart, bones, and soft tissues in the thoracic cavity. It helps identify conditions such as infections, heart enlargement, fluid buildup, trauma, and lung diseases.
🔍 How to Read a Chest X-Ray
- A - Airways: is the trachea central or deviated?
- B - Bones: check for fractures, lytic lesions, or asymmetry in ribs, clavicles, or spine.
- C - Cardiac: is the heart <50% of the thoracic width on a PA view? (Otherwise, consider cardiomegaly)
- D - Diaphragm: look for sharp costophrenic angles. Any air under the diaphragm?
- E - Everything Else: lines, tubes, soft tissue changes, and abnormalities like consolidation, pneumothorax, or effusion.
Normal vs Annotated Chest X-Ray
Compare a standard chest X-ray with an annotated version highlighting key anatomical landmarks in the mediastinum.

Normal PA Chest X-Ray: This is a standard posteroanterior (PA) chest X-ray of a healthy adult. The heart size appears normal (less than 50% of the thoracic width), lung fields are clear, and costophrenic angles are sharp - all suggesting no obvious pathology.

Annotated Mediastinal Structures: This annotated image shows key anatomical landmarks overlaid on a chest X-ray, including the heart chambers, great vessels (like the aorta and pulmonary arteries), trachea, and bronchi.
🧠 Quick Tips for Learning CXR Interpretation
- Always check the patient details and confirm it's a PA or AP film.
- Use a systematic approach (like ABCDE) every time.
- Compare both sides of the chest - symmetry is key!
- Review older images if available to assess changes.
- Don't rush - slow, structured observation leads to better accuracy.
Image credits: Wikimedia Commons (public domain / Creative Commons)
Blueprint Page
Explore the comprehensive blueprint for Physician Associates, covering all essential topics and resources.
Book Your Session
Enhance your skills with personalised tutoring sessions tailored for Physician Associates.
🌫️ Example Case 1: Lobar Pneumonia

Overview: This is a chest X-ray of a 67-year-old male patient with classic features of lobar pneumonia affecting the right middle lobe.
🩺 A>E Method for CXR Interpretation:
- A - Airways: trachea is central. Right main bronchus is visible. No deviation noted.
- B - Bones: ribs and clavicles appear intact. No fractures or lesions visible.
- C - Cardiac: heart size appears within normal limits for a PA film.
- D - Diaphragm: right hemidiaphragm appears slightly elevated, which may be reactive. Costophrenic angles preserved.
- E - Everything else: dense opacity seen in right mid-zone with sharp borders. No visible pleural effusion. No devices or lines present.
🔍 How to Spot It:
- Well-defined opacity seen in the right mid-zone - this represents lung consolidation.
- Sharp lobar borders indicate the infection is confined to a single anatomical lobe.
- Volume preserved - typical of pneumonia rather than collapse, where you'd expect volume loss.
🧠 Study Tip:
In lobar pneumonia, airspaces in one lobe become filled with pus or fluid, creating a white area on the X-ray. This can appear dense and sharply demarcated. Always assess for symptoms like fever, productive cough, pleuritic chest pain and bronchial breathing on examination.
Image: X-ray of lobar pneumonia by Mikael Häggström, M.D. – Wikimedia Commons (Public Domain)
🌫️ Example Case 2: Prominent Middle Lobe Pneumonia
Overview: This chest X-ray shows a right middle lobe pneumonia. The consolidation appears as a wedge-shaped opacity overlapping the right heart border - typical of lobar involvement.
🩺 A>E Method for CXR Interpretation:
- A - Airways: trachea is central. Main bronchi appear patent.
- B - Bones: no fractures or lesions seen in the ribs, clavicles, or spine.
- C - Cardiac: right heart border is partially obscured - a key clue pointing to right middle lobe disease.
- D - Diaphragm: right hemidiaphragm is visible and not elevated. Costophrenic angles remain sharp.
- E - Everything else: well-defined wedge opacity in the right mid-zone. No signs of pleural effusion or pneumothorax.
🔍 How to Spot It:
- Wedge-shaped opacity in the right mid-zone
- Silhouette sign: Loss of right heart border
- Middle lobe localisation due to anatomical position and border effacement
🧠 Tip:
Right middle lobe pneumonia is often missed on early review - look carefully at the right heart border. Clinically, it may present with mild breathlessness, cough, or low-grade fever. Confirm with auscultation and follow-up imaging if needed.
Image: Right middle lobe pneumonia by James Heilman, MD – own work. Wikimedia Commons (CC BY-SA 3.0)
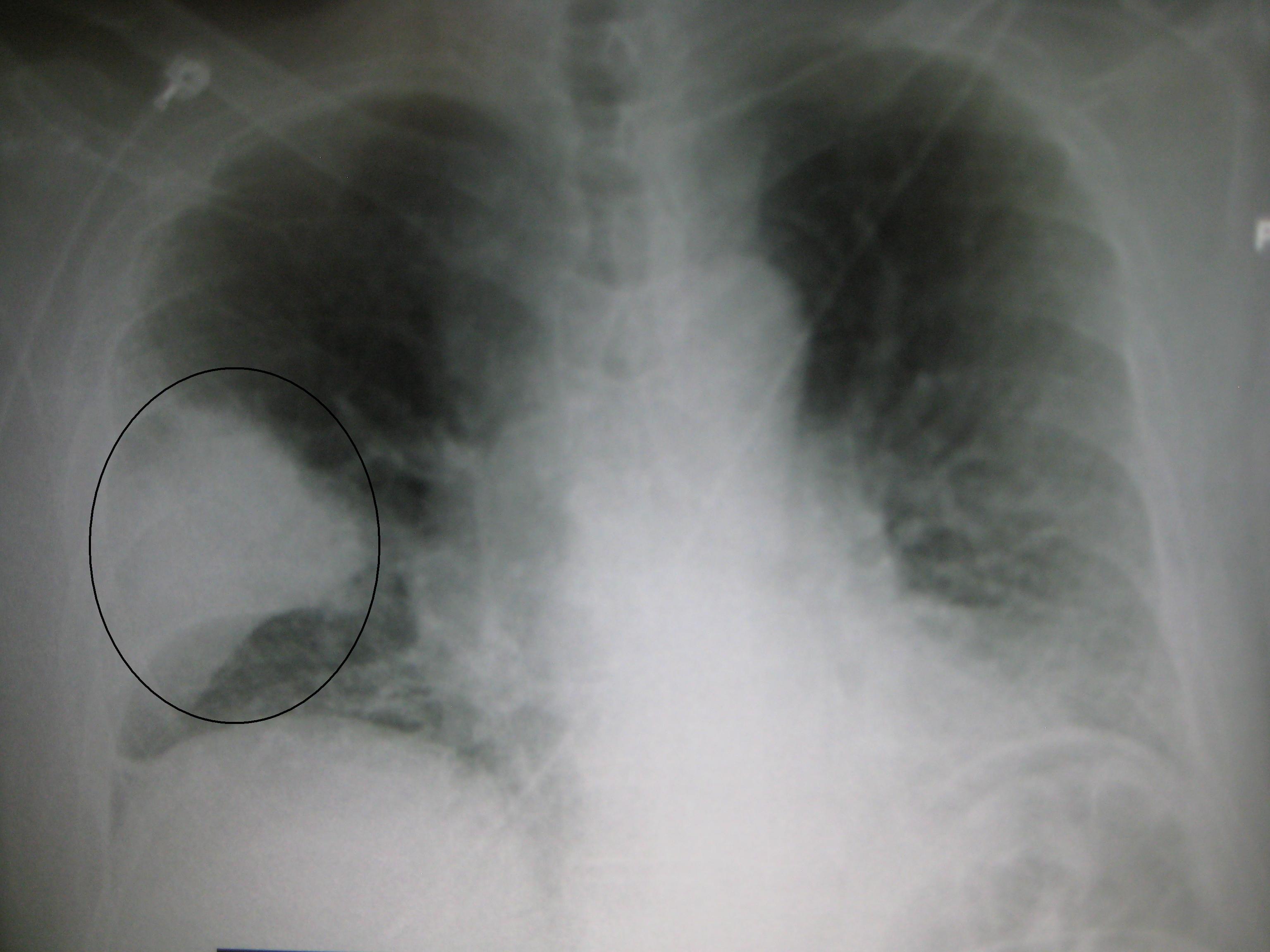
🌬️ Example Case 3: Tension Pneumothorax

Overview: This chest X-ray shows a left-sided tension pneumothorax. Air has accumulated in the pleural space, collapsing the left lung and shifting the mediastinum toward the right - a critical emergency.
🩺 A>E Method for CXR Interpretation:
- A - Airways: trachea is deviated to the right - a red flag for tension pneumothorax.
- B - Bones: no fractures or deformities noted in the ribs, clavicles, or shoulders.
- C - Cardiac: cardiac silhouette appears displaced to the right due to pressure from the pneumothorax.
- D - Diaphragm: the left hemidiaphragm appears flattened, another indicator of increased pressure.
- E - Everything else: left lung is collapsed and pulled medially. No lung markings in the periphery. The left side appears more black (hyperlucent) due to free air.
🔍 How to Spot It:
- Absent lung markings on the left side
- Visible pleural edge where the lung has collapsed inward
- Mediastinal shift to the right - key sign of tension
- Flattened diaphragm on the affected side
🧠 Tip:
A tension pneumothorax can quickly lead to cardiovascular collapse. If the patient is unstable, don’t wait for the X-ray - treat immediately with needle decompression in the second intercostal space, midclavicular line, followed by chest drain insertion.
Image: Annotated chest X-ray showing left tension pneumothorax
Source: Wikimedia Commons – Public domain
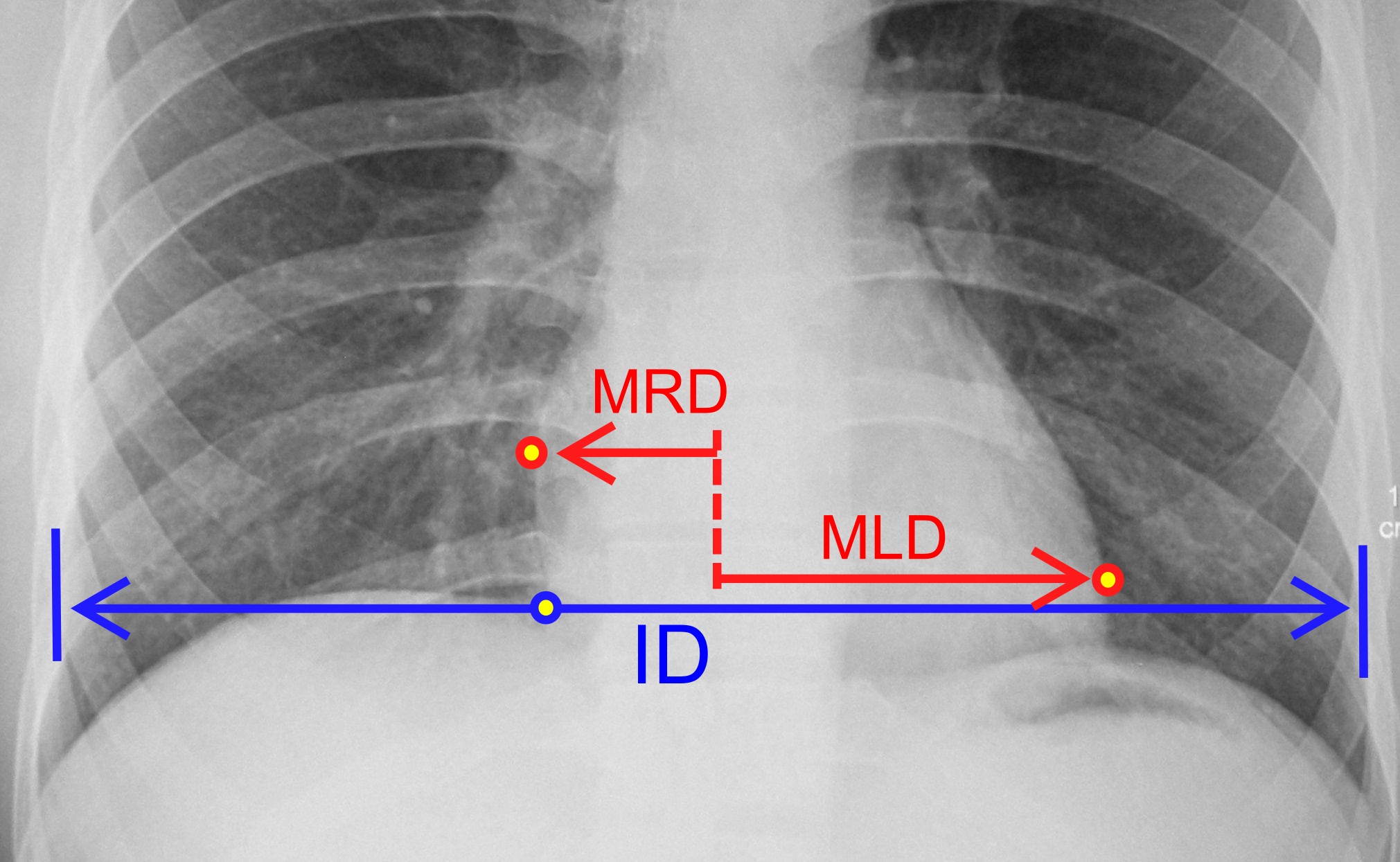
Cardiothoracic Ratio (CTR) – Normal vs Cardiomegaly
The cardiothoracic ratio (CTR) is a simple way to assess heart size on a posteroanterior (PA) chest X-ray. It’s calculated by comparing the width of the heart to the width of the thoracic cavity.
📏 How to Measure:
- MRD - Maximum distance from the midline to the right heart border
- MLD - Maximum distance from the midline to the left heart border
- ID - Internal diameter of the thorax (inside rib to inside rib)
Formula: CTR = (MRD + MLD) ÷ ID
Normal range: CTR ≤ 0.50 (i.e. the heart shadow should occupy ≤ 50% of the chest width)
Normal CTR: The heart takes up less than 50% of the thoracic width. This indicates normal heart size.
Image by Mikael Häggström, MD - Public domain via Wikimedia Commons.
🩺 A>E Interpretation (Normal CTR):
- A - Airways: trachea is central. No deviation seen.
- B - Bones: clavicles, ribs and spine appear normal. No fractures noted.
- C - Cardiac: heart size is within normal limits (CTR < 50%). Borders are sharp.
- D - Diaphragm: hemidiaphragms are dome-shaped. Costophrenic angles are clear.
- E - Everything else: lung fields are clear with no signs of consolidation, effusion, or pneumothorax.

Cardiomegaly: The heart shadow exceeds 50% of the thoracic width — suggesting an enlarged heart, often due to heart failure or dilated cardiomyopathy.
Image via Wikimedia Commons - Public domain.
🩺 A>E Interpretation (Cardiomegaly):
- A - Airways: the trachea is central with no signs of deviation. Main bronchi appear patent.
- B - Bones: no rib or clavicle fractures noted. Normal alignment of spine and scapulae.
- C - Cardiac: the cardiac silhouette is significantly enlarged. A pacemaker is visible in the left upper chest, with leads coursing into the right atrium and ventricle.
- D - Diaphragm: both hemidiaphragms are visible but slightly obscured on the left side. Costophrenic angles appear blunted - possibly due to underpenetration or effusion.
- E - Everything else: lung fields are generally clear. No evidence of consolidation, pneumothorax, or pleural effusion. Pacemaker leads are in situ. No tubes or devices are malpositioned.
🧠 Tip:
Always assess CTR on a PA view. AP (anteroposterior) films - often used in A&E or for bedbound patients - can make the heart look falsely enlarged due to magnification effects.
COPD & Emphysema – Chest X-Ray Examples
These chest X-ray images highlight important radiographic signs of COPD and emphysema. Recognising these patterns can help Physician Associates and students interpret imaging confidently in clinical practice.
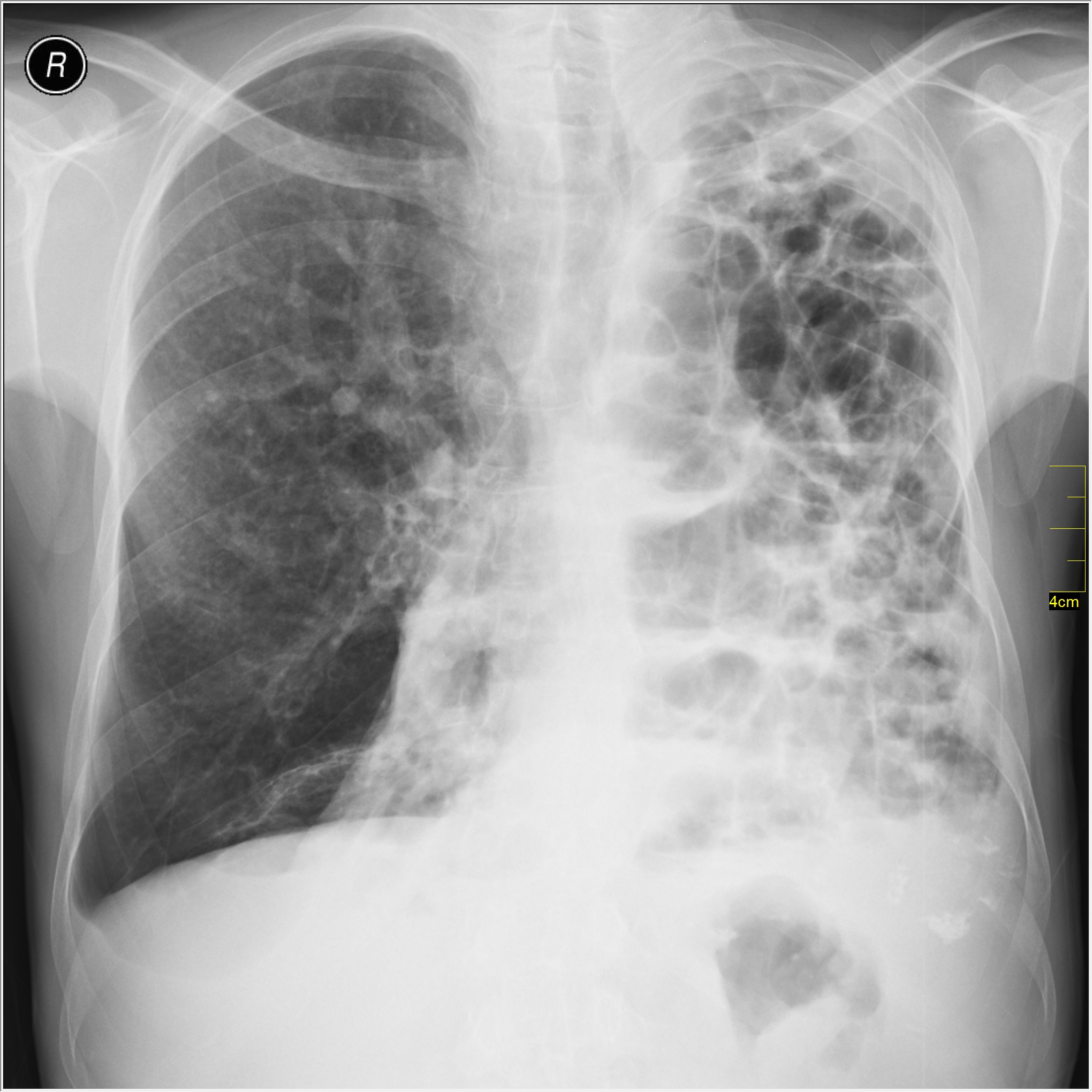
📸 Bullous Emphysema
Visual clues: Large, air-filled cystic areas (bullae) replacing lung parenchyma, with thin surrounding walls.
Interpretation: These bullae reduce functional lung area and do not contribute to gas exchange - increasing risk of rupture and pneumothorax.
Image by Nevit Dilmen – Public domain, Wikimedia Commons (2011)
🩺 A>E Interpretation:
- A - Airways: trachea central; bronchi visible.
- B - Bones: no fractures; ribs and clavicles intact.
- C - Cardiac: heart displaced due to large bullae.
- D - Diaphragm: flattened, consistent with hyperinflation.
- E - Everything else: multiple large bullae, especially on the left; reduced lung markings; no effusion.
Image: Public domain via Wikimedia Commons

📸 Severe COPD – PA View
Visual clues: Hyperinflated lungs, flattened diaphragms, narrow heart shadow, and increased radiolucency.
🩺 A>E Interpretation:
- A - Airways: trachea is midline.
- B - Bones: ribs are horizontal with increased intercostal space.
- C - Cardiac: narrow heart silhouette due to lung hyperinflation.
- D - Diaphragm: both hemidiaphragms are low and flat.
- E - Everything else: hyperlucent lungs with poor vascular markings. No consolidation or effusion.
Image by James Heilman, MD – Wikimedia Commons
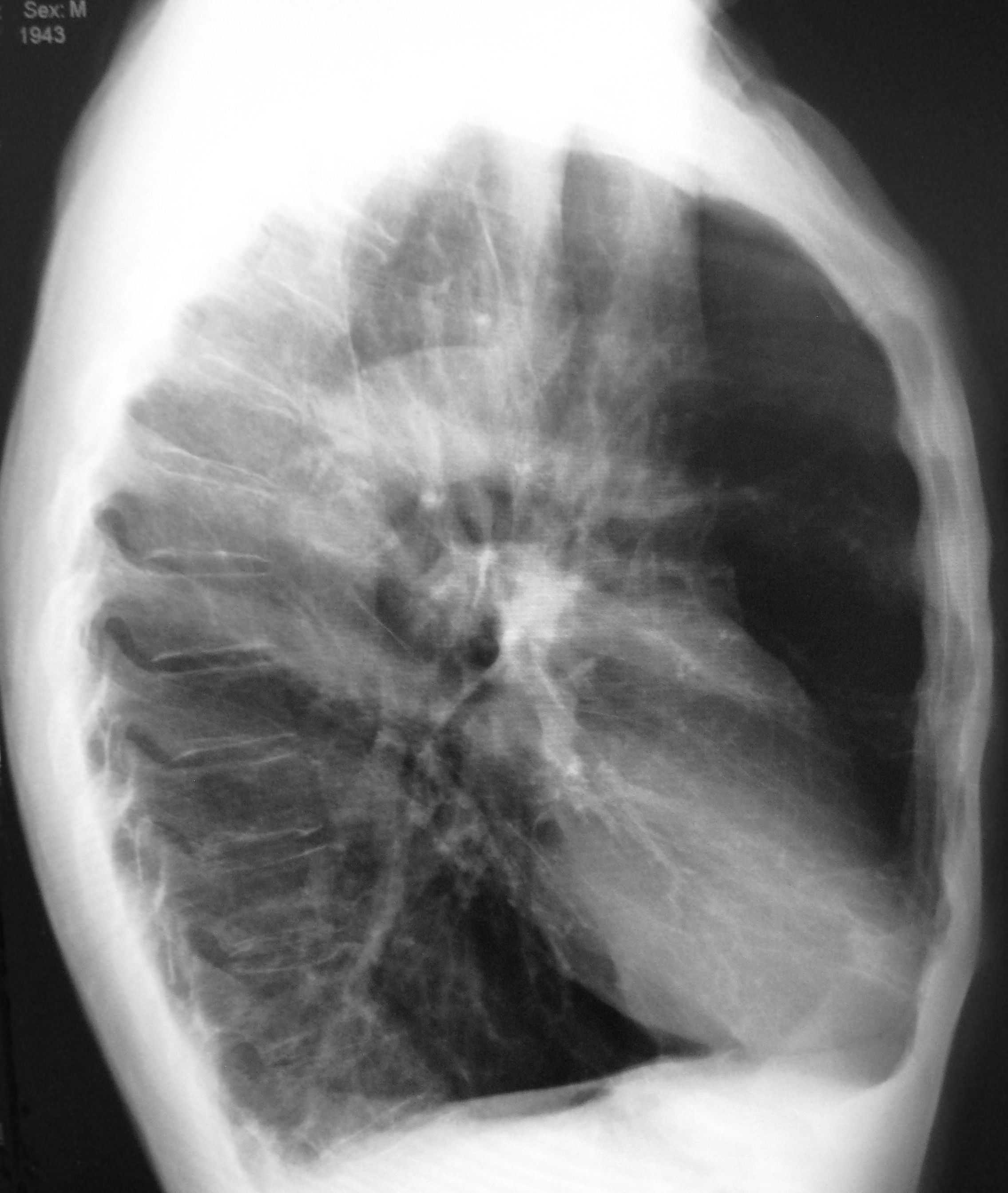
📸 Lateral CXR - Emphysema
Visual clues: Barrel-shaped chest, increased anterior-posterior diameter, flattened diaphragm, and enlarged retrosternal air space.
🩺 A>E Interpretation:
- A - Airways: trachea is not clearly visible in lateral but appears patent.
- B - Bones: vertebrae and ribs intact. No fractures.
- C - Cardiac: compressed heart silhouette anteriorly.
- D - Diaphragm: very flat with increased space between lung and dome.
- E - Everything else: hyperinflation evident with prominent retrosternal air space. No masses or fluid.
Image by James Heilman, MD – Wikimedia Commons